We speak with a governor, a former C.D.C. director, a pandemic forecaster, a hard-charging pharmacist, and a pair of economists — who say it’s all about the incentives. (Pandemillions, anyone?)
Listen and subscribe to our podcast at Apple Podcasts, Stitcher, or elsewhere. Below is a transcript of the episode, edited for readability. For more information on the people and ideas in the episode, see the links at the bottom of this post.
* * *
A few months ago, we tried something different: a conversational, question-asking episode between me and Angela Duckworth, the University of Pennsylvania psychologist who wrote the book Grit. We thought it might make a good spinoff podcast. You agreed. And so we’ve done it. Our new podcast is called No Stupid Questions. You can go ahead and subscribe now on Apple Podcasts or Spotify or Stitcher — wherever you get your podcasts. We’ve already posted a preview, and starting May 18 we’ll be putting out a new episode every Sunday evening.
Also: announcement No. 2. Something the Covid-19 pandemic has us wondering is: What’s college going to look like this fall? Maybe you are wondering that too. If you are a student or parent or college faculty or staff member with a question or concern or maybe an insight, we would like to hear from you for possible inclusion in an upcoming episode. Use the voice memo app on your smartphone and e-mail the file to radio@freakonomics.com. Please include your name and where you live.
* * *
Stephen J. DUBNER: Hello, it’s Stephen. Can you hear me?
Gina RAIMONDO: Yes. Hi. Good morning, Stephen.
DUBNER: Good morning. How are you, Governor Raimondo?
RAIMONDO: I’m hanging in there.
DUBNER: How’s your life these days generally?
RAIMONDO: Pretty calm. Not much going on. Everything’s in order.
Gina Raimondo is the governor of Rhode Island, which had its first Covid-19 diagnosis on March 1st.
RAIMONDO: We were one of the first 10 states in the U.S. to have a positive case. We’ve been at this for a while.
More than 7,000 people have since tested positive in Rhode Island, and over 200 have died. I spoke with Raimondo on April 19, a Sunday morning.
RAIMONDO: So I think that we are probably a couple of weeks away from our peak. We’re still climbing up the curve.
Like the rest of the U.S., Rhode Island has been sheltering in place. Only essential businesses are open and the economy has cratered.
RAIMONDO: There’s a lot of people now who — and maybe I’ll put you and a lot of my friends in this category — their lives have been inconvenienced, surely, but they’re not devastated. They grab their computer and their phone. They work from home. They’re still getting a paycheck. That isn’t the majority of Rhode Island right now. The majority of Rhode Island really is struggling.
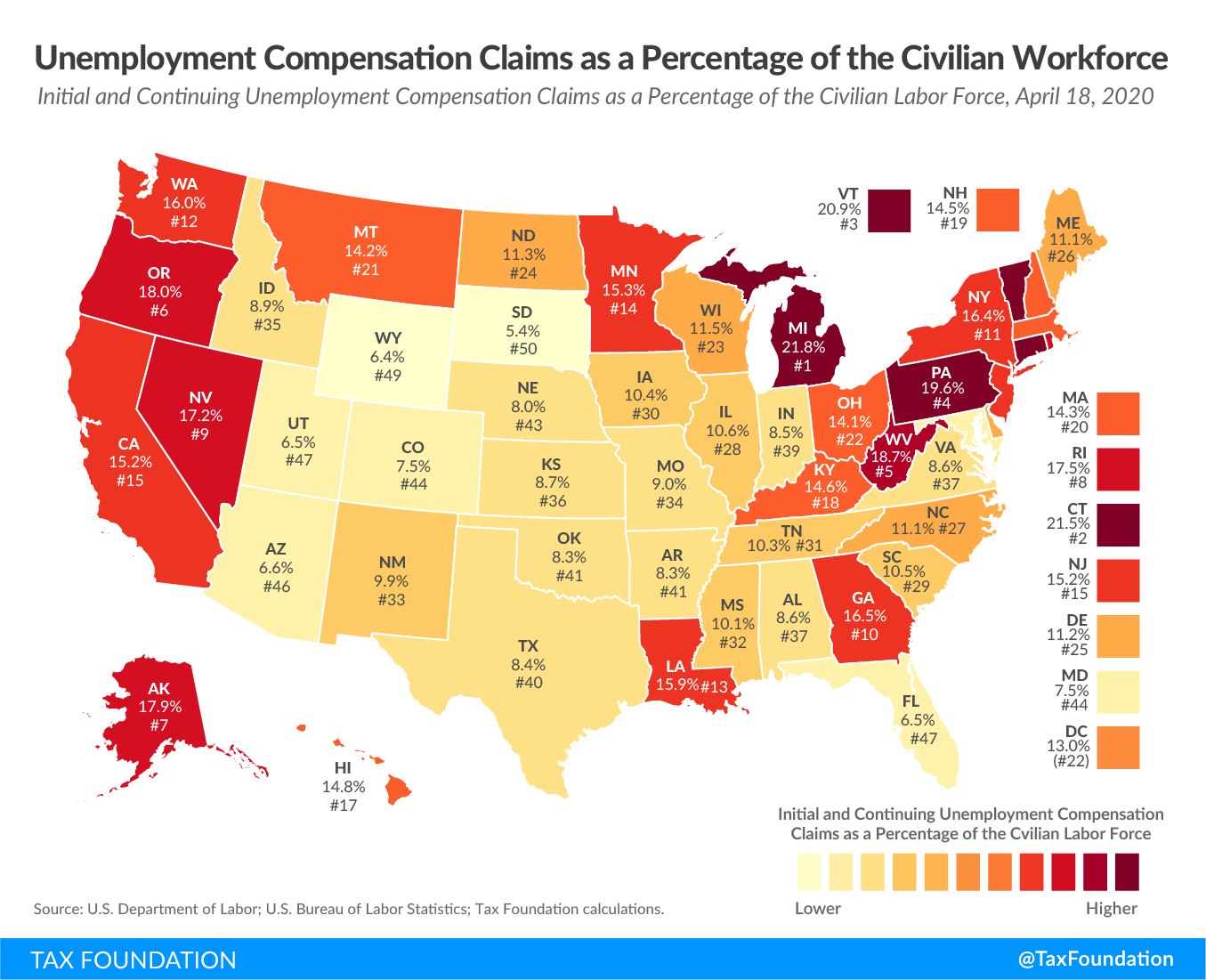
With a population of just around one million, Rhode Island has had 170,000 people file for unemployment. That puts it in the top 10 nationally for the largest unemployed share of the civilian workforce.
{kind=link}
RAIMONDO: So I’m obsessed, with every minute of every day thinking, “What’s it going to take to safely reopen the economy? How can I get the most people back to work the fastest, as safely as possible?”
Rhode Island’s current stay-at-home order is set to expire on May 8th, but new infection rates are still high.
RAIMONDO: There’s no good options. I’m choosing between bad option number one and bad option number two. And all of the work that we’re doing is to make this a bit less bad for people: minimize death, minimize the virus, minimize economic hardship.
This dilemma is shared by governors across the country, by elected officials around the world. A few U.S. states have begun at least partial reopenings. Others plan to reopen soon, while some are likely to extend their shutdowns. That will of course only deepen the economic cataclysm.
DUBNER: So there is a chance that restarting the economy, whenever and however it happens, will fail — given inadequate testing and our limited knowledge of the virus to date. What would it take for you to admit failure and return to lockdown if that were the case?
RAIMONDO: That is the worst possible outcome. When I reopen, I’m going to have a set of metrics based on science and fact which will say if your infection rate starts to look like this, if your hospitalizations are doubling this quickly, then you have to hit the brakes again. The whole point of all of what we’ve gone through is that you won’t again have to do a wholesale shutdown.
Consider the 1918 influenza pandemic. It killed roughly five million worldwide, around 675,000 in the U.S. Our population then was about one-third what it is today — so the modern equivalent of around two million people. The 1918 pandemic hit the U.S. in three waves: spring, fall, and winter. The first wave wasn’t that terrible; the third was bad; but it was the second that easily killed the most people. This fact, if you are a governor, weighs heavily on your decision of when and how to reopen the economy.
RAIMONDO: There is risk. There’s no risk-free option here.
Today on Freakonomics Radio: how can that risk be mitigated? We discuss Covid-19 exit strategy with a former head of the Centers for Disease Control; a pandemic forecaster; a hard-charging pharmacist; and, of course, a couple of economists, who have economist-type ideas:
Steve LEVITT: So you could imagine we could put something like $1 billion a week into this lottery.
* * *
Covid-19 has so far killed more than 50,000 people in the U.S. I asked Gina Raimondo to describe what it was like when the disease first hit Rhode Island.
RAIMONDO: I cannot describe to you the chaos in the first few weeks of this. We were so poorly prepared for this crisis. The federal government was absolutely not ready. The federal stockpile wasn’t where it should have been. They moved much too slowly to ramp up manufacturing of P.P.E. and testing. So we were just scrambling for too long and we’re behind. We’ve been playing catch up from day one. Because we were one of the first states to have a case, within a week, I had banned large gatherings. I was one of the first states to do that. Closed schools, one of the first states to do that. At the time, I got a lot of pushback. People said, “It’s not necessary. You’re overreacting.”
DUBNER: Pushback internally, externally, from where?
RAIMONDO: Constituents in Rhode Island. I remember the first call I had to have with our bishop, which was a difficult call. And I asked him if he would please consider suspending Sunday mass. And at the time— and he was excellent and cooperative, but reluctant at that time. And, of course, eventually he did do what in hindsight was clearly the right thing. Everybody cooperated. And as a result, now we— it worked. We never had the extreme spikes. Our healthcare system has never been overwhelmed.
Raimondo had two temporary hospitals built, with a third on the way, totaling 1,000 beds; so far they haven’t been needed.
RAIMONDO: I mean, it’s still all horrible. The amount of pain and suffering and economic hardship is so extensive and extreme. But two weeks ago when I was looking at our models, we were looking at a need for six or seven thousand hospital beds. That was a scary place to be.
DUBNER: Those models persuaded a bunch of governors to take extreme action. Do you have any reservations now about having followed those extreme models, or do you think it was ultimately the right move?
RAIMONDO: Ultimately the right move.
DUBNER: In late March, when it was becoming clear that New York was a hotspot, you were sending police officers and National Guard troops to intercept cars with New York license plates to tell people that they had to self-quarantine for two weeks. You sent police to the main airport and the train stations. They went door-to-door in resort towns looking for New York plates. So tell us about that incident, what you did right there, maybe anything you did wrong.
RAIMONDO: Yes. So I would do that again on the basis of all the information we were receiving. As I looked at other communities outside of Rhode Island, the rate of infection was so much higher than what we were seeing and I had Rhode Islanders in coastal towns calling me, saying, “Hey, Governor, when we go to Stop and Shop, it’s all out-of-state cars. Help us.” They were afraid. I had to respond to that.
Her response provoked a response from New York governor Andrew Cuomo:
Andrew CUOMO: If they don’t roll back that policy, I’m going to sue Rhode Island. Because that clearly is unconstitutional.
RAIMONDO: In retrospect, I should have not singled out one state. So if you recall, I did an executive order one day.
DUBNER: And then you later included the other states, right?
RAIMONDO: And then the next day, I included every state. So were I to do it all over again, I would’ve not done the New York executive order, followed by everyone. I would have treated everybody the same. By the way, in all of the hyperbolic headlines — “Rhode Island Governor, Police State, Lockdown” — we never closed our borders, right? We were welcoming to anyone who wanted to come here, you just had to provide us with information so we could keep you safe and the people of Rhode Island safe.
DUBNER: Did you think about closing your borders?
RAIMONDO: No. No, I didn’t.
DUBNER: Is it legal?
RAIMONDO: It’s a good question. It would depend. I’d say probably not. That would be a real interference with interstate commerce.
DUBNER: You’re being asked to come up with a strategy for restarting the economy, but without what I would think is the testing capability that experts say are necessary, without good information about even what behaviors will or won’t spread the disease at this point. So do you feel— I mean, bad and worse is one way of describing it. Impossible, I guess, is another way to describe it.
RAIMONDO: So you’re absolutely right, by the way. The key things are: you have to rely on the data that you can get your hands on. So in my discussions, the loudest voice in the room is my public health advisor. All that matters is that you try your best on a daily basis with the facts before you to make the best decision you can. And, here’s the hard part for politicians: be willing to change. So, as the facts change, as our information about the virus changes, people like me have to be willing to say, “I’m changing. I was wrong.”
DUBNER: So I’m guessing your lockdown exit strategy has different phases of reopening, like most plans. What do you see as the easiest and hardest parts of society to reopen?
RAIMONDO: So it will be a phased plan and we all as a country have to get ready for social distancing for the next year. Now, what that looks like in the beginning will be crowds of fewer than five or 10 people. Months from now, it will obviously be bigger crowds.; it could be 50 or 100. But the days of hand-washing, mask-wearing, and social distancing are here to stay until we have a vaccine. I don’t think people really get that, so I say it often. The hard call for me is school. That’s a really tough call for me right now: what to do about school.
DUBNER: I mean, thank God kids are not particularly susceptible. That’s a huge blessing of this weird virus, right?
RAIMONDO: Huge. That’s huge. But a lot of them live with grandma and grandpa, aunts and uncles. Custodians in schools are often over 50 or 60. Lots of teachers are over 50 or 60. None of us has ever gone through this before. It’s hard to call somebody and say, “How would you handle it?” Because none of us has gone through it.
Julie GERBERDING: When I first saw the number of patients being admitted to the hospital in Wuhan, China, I knew that this was going to be a bad outbreak.
And that’s someone who has been through a few pandemics.
GERBERDING: But I think the moment that I really grappled with the transmissibility was watching that cruise ship in Japan and seeing how that disease spread so quickly to involve so many passengers on that boat.
That’s Dr. Julie Gerberding.
GERBERDING: I was the director of the U.S. Centers for Disease Control and Prevention, or C.D.C., from 2002 to 2009.
Gerberding is an infectious-disease expert. These days, she is the chief patient officer for the pharmaceutical firm Merck. And what did she think when she first saw how transmissible Covid-19 was?
GERBERDING: That was not SARS that I knew in 2003. It was SARS that was much more transmissible at a community level.
Gerberding has been through not only SARS, but the H1N1 outbreak in 2009, MERS in 2012, and her career began back in the midst of H.I.V./AIDS. Pandemic management from the public health side, she says, comes in three phases. Number one:
GERBERDING: Phase one is really early detection. And in the case of this new coronavirus, we had fairly early translation of the fact that there was something new and dangerous going on in China. And in Wuhan, I would say they used some of the most draconian methods possible to contain the outbreak, things that would probably be impossible in a number of other more westernized countries. But nevertheless, they made a heroic effort to really slow the spread and try to minimize transmission beyond the original epicenter.
But that, plainly, didn’t happen. Once a contagion spreads to other parts of the world, you’re in phase two:
GERBERDING: Which is the mitigation phase. You can’t stop it, but perhaps you can slow it down. So that’s what has led to all these social-distancing efforts. But sometimes we forget there are two parts to mitigation. One part is really taking the social-distancing measures and all that implies seriously, but the other is making sure that we do it sustaining essential services. So how we think about balancing the need to protect people and slow down the impact on our health system and at the same time maintain our social services — that’s a tough balance to get right.
That balance is what we’re all struggling with these days. And what’s next?
GERBERDING: The final phase is, of course, recovery, and unfortunately we’re not quite there yet in most communities around the world. So we are not really developing the firm policies for how we will try to come out of this, in part because we don’t really know what’s going to happen next. Is this going to resolve as our social-distancing measures really take hold? Or are we going to see a second wave that could be as bad or worse?
Chris MURRAY: So back in the SARS-1 epidemic, all the models suggested there would be a second wave for SARS.
That’s Chris Murray.
MURRAY: I’m the director of the Institute for Health Metrics and Evaluation.
I.H.M.E. is a research group at the University of Washington whose Covid-19 forecasting has driven much of the public-policy response to date, including White House policy.
MURRAY: And of course, the vast majority of the world was susceptible. There wasn’t a second wave. We don’t really know why. And it would be great if that occurs now, but hope is not a strategy. And given what we’ve seen about how much more widely spread Covid is than SARS-1, we should expect that the risk of a second wave is great. The vast majority of the U.S. will be susceptible. And that means that we need to be better prepared in terms of testing, contact tracing, isolation strategies.
These are the measures most people agree are key to any sensible lockdown exit strategy: testing, contact tracing, and isolation strategies. But — much easier said than done. For one thing, even though the death rate has slowed, the disease is still very transmissible and somewhat mysterious. It is, after all, a novel coronavirus. It’s attacking the body in ways that the most expert doctors and scientists are still trying to figure out. One phrase you often hear when you speak with these people: “It’s the fog of war,” they say. For Julie Gerberding, one close equivalent was the AIDS outbreak:
GERBERDING: In some sense, my career is bookended by two pandemics. When I was a very junior clinician and H.I.V. was first emerging in San Francisco, I had a whole roster full of very, very sick patients, mostly young men, with what we now recognize as AIDS, but at the time, we did not have any idea what this disease was. We just had very, very sick and dying people. And they had bizarre, complicating infections and cancers. And it was a nightmare. And all we could really do for our patients was to just care about them, try to help them be comfortable and cope with their illness.
Gerberding’s own research was focused on trying to understand how H.I.V. could be acquired through blood exposure. Some AIDS patients were not receiving treatment because many doctors were fearful of contracting H.I.V.
GERBERDING: Back then, we had no idea how big the risk was. So I can only imagine what it’s like to be on the frontline of this coronavirus and recognize the hazard that health workers are experiencing, but also their frustration with it, by not having the protective equipment they need to feel confident in their safety.
Gerberding sees another parallel between Covid-19 and AIDS:
GERBERDING: Both of these situations started in an environment of complacency. When H.I.V. emerged, it took us a long time to even recognize that it was an infectious disease because we had been lulled into this false sense of security that we had antibiotics and vaccines and we were really enjoying the end of the infectious-disease threat era. And AIDS sobered us up very quickly. That: No, no, no.
We’ve had a number of scary things happen in the last several years with infections emerging from contact with animals, including bats, civets in the case of SARS in 2003, and so forth. So when the coronavirus emerged in China last year, I think a lot of people thought, “Well, it’s over there. It’s not us. We’ve seen this before. Yes, we had a SARS outbreak in 2003 and it was frightening for a while, for eight months or so. And 8,000 people were infected and 800 of them died.”
Those aren’t U.S. numbers; those are global numbers. Again: roughly 8,000 people worldwide contracted SARS, and 800 died. As of this recording, roughly three million people are thought to have contracted Covid-19, with more than 200,000 dead. Different countries have responded differently. Sweden, for instance, has not shut things down; even schools and restaurants remain open. Their goal is to achieve what’s called “herd immunity” by letting the virus work its way through the population. And on the other end of things: Singapore used what you might think of as Orwellian surveillance to identify and isolate people who’d been exposed to the virus.
GERBERDING: Those are two polar extremes of the equation, and I don’t think the jury’s in yet in terms of which ultimately proves to be the best overall approach. Each government has taken a look at its local situation. In Korea, for example, given that the majority of the early cases were all linked to a particular religious group, the country could go in and really concentrate on finding the people who were members of that congregation and getting them evaluated, tested, isolated if they were positive, or quarantined if they were exposed.
MURRAY: If you want a success story right now—
Chris Murray again, from I.H.M.E.
MURRAY: I think it’s New Zealand, which had community-based transmission, had a broad-based shut down, and has got transmission to near zero at this point.
RAIMONDO: In an ideal world, you would want to know where everyone is at all times.
Rhode Island governor Gina Raimondo again:
RAIMONDO: However, in the United States of America, we don’t live, and frankly, I don’t want to live, in that kind of a state. So we have to protect privacy and civil liberties and also, in that context, put in place the most rigorous contact-tracing system we can find.
Contact tracing meaning you inform people who’ve interacted with someone who’s tested positive so that they too can self-quarantine. I asked Raimondo what’s the best middle ground or compromise she’s seen for contact tracing.
RAIMONDO: Well, I can tell you what we’re thinking about: a lot of consumer choice, a lot of opting in, not forcing people for some of the more invasive options, making it easy, providing incentives, and just making the case to people that if they do provide their information, it will be secure. It’s never going to get into the hands of a business; it will be destroyed appropriately.
But Rhode Island isn’t there yet; they are not ready to lift the lockdown. Some states are — Oklahoma, Georgia, and South Carolina began the process last week — and that should provide some useful epidemiological data. Meanwhile, in states where political leaders aren’t ready to reopen, there have been protests.
RAIMONDO: People are angry, tired, anxious, sick of being cooped up. And, by the way, they should be. How could you not be, after being locked in your house for a month? But the test of leadership for people like me is whether we can lead people through that anxiety to a place of realizing that it’s in their best interest too, to follow the rules.
DUBNER: So how do you do that if I, let’s say, run a small restaurant and I’ve had zero dollars for the past five, six, seven weeks? And I know that there is a federal plan that’s not working very well. It’s already tapped out. It was hard to get. Let’s say I didn’t get any of that. And I get you on the phone and I say, “Governor Raimondo, I understand. I want to do my part. But you’re killing me here. You’re killing me.” What do you say to me there?
RAIMONDO: I know, and I’m sorry. There’s no other option. If I let you open right now, nobody would show up anyway because they’re afraid, and it would just make the problem worse. Because if you open now, everybody gets sick, we start flying back up the curve, we’ll be in this mess longer. So although it stinks, hang in there with me for a couple more weeks, because I want to get you back in business as fast as I possibly can. But unfortunately, until there’s a cure for this disease, we’ve got to take it slow.
A “cure” meaning a therapeutic treatment, which has remained elusive, and/or a vaccine. Scientists around the world have more than 70 different vaccine candidates in progress, with a handful already in clinical trials. Julie Gerberding again:
GERBERDING: This should be a virus for which we can create a vaccine. Merck has an animal-health business, and because coronaviruses are common across many, many animal species, we actually do have some vaccines that have to do with other coronaviruses and other animal species. So I feel very confident that we will end up with a vaccine. The question is, how fast?
Typically, a new vaccine can take about 10 years.
GERBERDING: With vaccines you have to be concerned about two things. One is the length of protection, if any, and second, the safety, because if you’re going to deliver a product to someone who’s really healthy, you want to be absolutely sure that it is as safe as possible. So the testing for vaccines has to occur over a much longer arc of time, long enough to tell whether or not protective immunity occurs and lasts long enough to be practical from a public-health perspective. And studies have to be long enough so that the full spectrum of safety concerns can be observed and addressed in the process of the clinical development.
But with a public-health threat of this scope, the norms may be adjusted to accelerate things. The Trump administration said we can expect a vaccine in 16 or 18 months. How realistic is that?
GERBERDING: I’m optimistic we’ll have a coronavirus vaccine, but I’m respectful of the timeline and then the scale. It’s not going to be helpful to have a vaccine to protect some people in one country or a few countries. We’re going to need the capability of producing the vaccine so that we have equitable access among all the people who need it. And that is an order of magnitude that we have never achieved in the history of the world.
No one knows how the search for a Covid-19 vaccine or treatment will play out. History does provide a lesson or two. After four decades, there is still no H.I.V. vaccine — but there are therapeutics that have rendered AIDS no longer a fatal disease. Polio, meanwhile, has a vaccine — which is wonderful, because scientists weren’t able to come up with a viable treatment. How does this inform our thinking on Covid-19? In the absence of a vaccine (for now) or a therapeutic solution (so far), the main weapon is reducing the spread of the virus. And that is hard to do without more testing.
RAIMONDO: Yeah. Testing is the key.
Governor Raimondo again.
RAIMONDO: In a magical world— imagine if I had enough tests where every day everyone, before they walked into work, could be tested and have a result within five or 10 minutes. I mean, in that world we could reopen tomorrow. Now, obviously that is not the world in which we live, but my point is testing is really a key piece of the puzzle. We’re doing more than 2,000 tests a day. So more than 2,000 per million puts us on the high end of testing. I think, however— I know we need to be doing multiples of that per day before we can start reopening the economy.
So why isn’t there more testing?
* * *
I recently called up Steve Levitt, my Freakonomics friend and co-author. He’s an economist at the University of Chicago — which, like all schools, has moved to remote teaching.
DUBNER: So, Levitt, how’s your sheltering in place going, generally?
LEVITT: Not too bad. I’m lucky I didn’t lose my job and I’m healthy. I don’t really like people that much in the first place so I don’t mind being isolated. So I know other people are really suffering, but I’ve been super lucky.
DUBNER: So let me ask you this: How useful would you say that economists have been so far during this pandemic?
LEVITT: I think economists didn’t really have a very big role in the beginning and the middle, in the sense that it was really more like a medical issue or a policy issue. But I think on the exit from quarantine, economists can be really important because the tradeoffs we’re talking about here are the kind of tradeoffs that regular people don’t think about very much, like the tradeoff between life and death versus economic activity. I think there’s also just a lot of room for economists here to be sensible guides as we think about what will work and what won’t work.
Levitt, like everyone we’ve already heard from, agrees that an exit from quarantine won’t work without a lot more testing.
LEVITT: I think there’s been an enormous failure on the part of the government in not getting testing in place. That any sensible plan we have now requires millions and millions of tests per day, far more than the capability we have, and really some of the plans suggest 20 million tests a day.
The U.S. is now performing around 200,000 tests a day.
Zack COOPER: The economy’s losing $16 to $19 billion a day, half a trillion, nearly, a month. It would just seem like the right thing to do would be to just dramatically scale up the investment.
And that is Zack Cooper, a healthcare economist at Yale. He’s part of a group of economists who routinely collaborate with policymakers.
COOPER: Yeah, so this is reaching out to folks on the Hill, in the Senate and the House, folks in the executive branch, at the White House, at H.H.S.
Cooper, like Levitt, was quickly convinced that lack of testing was a huge problem.
COOPER: So I think right now, we’re in the fog of war, where we just don’t even know how widespread Covid is across the population.
If you’ve been keeping up with the news, you’ve probably heard about several studies that do claim to measure the spread of Covid-19. But most of these studies aren’t very reliable. They don’t measure a truly random sampling, like the studies that use Facebook to solicit people — people who may already be feeling sick. Or the studies that test people who are shopping at a grocery store — people who may be less isolated than the average person.
COOPER: So I think the best studies we actually have, are some of the studies that look at the prevalence of Covid among pregnant moms.
That is, women in hospitals — New York, in this case — who are having babies.
COOPER: That’s probably the most reliable estimate of the prevalence of Covid in the population, because there is a group of folks who are very, very health-conscious, were probably avoiding going out, whereas if you start testing shoppers, that group just looks different than the folks who are sitting at home.
And what was the Covid incidence among these women?
COOPER: You’re seeing in New York that those numbers are on the order of like 15 percent.
New York, keep in mind, has been the Covid epicenter. Does that mean the numbers elsewhere are much lower? No one really knows yet. That’s why a pair of Dartmouth researchers — the mathematician Daniel Rockmore and the political scientist Michael Herron — have proposed a truly random testing of just 10,000 Americans that they claim would predict how many people are infected. Another way to know, of course, would be to have much higher testing capacity.
How will this happen? Let’s first talk about what Covid tests are and what they can do. There are two kinds of tests: a molecular, diagnostic test, usually taken with a nasal swab, that looks for the virus itself; and a blood test that looks for antibodies, which signals that a person has already been fighting the coronavirus. The idea — the hope — is that a positive antibody test means that you’ve got immunity. Germany, for instance, is considering immunity certificates for people who test positive for antibodies. But former C.D.C. official Julie Gerberding says that science isn’t clear yet.
GERBERDING: First of all, many of the tests that are now becoming available for antibody testing are not performing very well. And by that I mean they are giving false positives and false negatives. So it’s hard to interpret unless your test is one of those that has been done by a laboratory in a major medical center that’s undergone this sophisticated approval testing, or has come out of the F.D.A. as an emergency-use evaluation test.
Second problem is that we don’t know what the antibody result means. You might have an antibody, which means you’ve been exposed to the virus, but it doesn’t necessarily mean you’re not going to get it again because we don’t know if the antibodies are protective or not. I hope they will be. Usually, after infectious diseases, you do see the antibodies confer some protection, but not always. I think some people have the misunderstanding that if we could know someone has an antibody that would be a return-to-work ticket. That’s just not really the case. And if you think about H.I.V., for example, everybody with H.I.V. infection has antibodies, but nobody is cured or protected because of those antibodies. So we have to know the answer to the meaning of the antibody tests before we can really decide who should be tested and when.
The F.D.A. has granted emergency-use authorization for more than 60 versions of the Covid test from multiple manufacturers. Most of these tests are diagnostic, but a few are antibody tests. The first such authorization went to the C.D.C. on Feb. 4.
COOPER: I think there was a recognition that initially there was way too much regulation of testing and that that regulation was really choking off production. And they loosened the reins quite a bit, which allowed a lot of manufacturers to get expedited review and approval of their testing.
But, as we’ve been hearing, there’s still not nearly enough testing available. Why not? One reason is that the U.S. medical-supply chain, much of which runs through China, has been significantly disrupted. But Cooper says that’s only part of the answer.
COOPER: So I think there are two market failures. The first is just the sheer scale of the externalities associated with testing, meaning that we are literally paying way too little per test we perform.
That is, there should be stronger financial incentives to produce test kits, given how valuable testing is to society.
COOPER: The second is we’re looking to scale up huge numbers of tests on a scale that we’ve never done before, for a problem that’s going to dissipate pretty dramatically in 18 to 24 months. You’re asking all of these firms to put out more than they ever have, and bear the cost of doing so, without the ability to recoup those costs the way we normally think about costs being recouped over fairly long periods.
In other words, if this were your company, would you invest a lot of money in ramping up to make millions of a product now for which there may not be much demand in a year or two? If there’s a Covid-19 vaccine, there won’t be nearly as much need for a Covid-19 diagnostic test.
COOPER: So the solution to that is just paying them a ton to do that now.
And just how much is a ton?
COOPER: There just aren’t that many production issues that $250 billion can’t solve.
That is precisely 10 times what Congress just directed toward coronavirus testing in the latest relief package. But as Cooper points out: if the economy is losing between $16 and $19 billion a day, and if greater testing capacity could help restart the economy 30 days earlier, that’s a savings of roughly $500 billion. Which makes $250 billion for testing look pretty affordable. Cooper has a plan to ramp up production. The first thing to do is get prices aligned.
COOPER: We basically need the federal government to set a payment rate for Covid tests that applies to all parties in the healthcare system. Right now, you’ve got Medicare paying a different rate from Medicaid, which is paying a different rate from each private insurer. That needs to change because it just drives contracting frictions.
As you likely know, economists aren’t typically in favor of fixing prices — at least under normal market conditions. But plainly, these aren’t those. So that’s one solution: a single price.
COOPER: The second is, that payment rate really needs to be quite high, sort of on proportion to the social value of testing. I think in many ways, it would be almost impossible to underspend on testing right now.
At the outset, the Centers for Medicare and Medicaid Services, C.M.S., was paying between $30 and $50 per Covid test. It has since raised payments to $100 per test.
COOPER: Now, I actually think they should be paying dramatically more. I think if you’re paying $250 per test, that wouldn’t be crazy. Frankly, I think if you’re paying a $1,000 per test, given the scale of harm we’re facing, that itself wouldn’t be crazy either.
But price alone, Cooper says, won’t increase the supply of test kits.
COOPER: There are going to be supply-chain problems in the production of tests and in the material necessary to support testing. One of things that we’ve called for is using the Defense Production Act to guarantee the production of some of the inputs to testing, like re-agents and like swabs.
In case you haven’t been following the news lately and reading about the Defense Production Act:
COOPER: So the Defense Production Act broadly allows the federal government to steer the behavior of private firms to produce necessary supplies. And then there’s a mechanism for those firms to get reimbursed. So the crude way to think about it is we say to G.M., “Look, G.M., we are going to force you into the production of Covid-testing swabs.”
The Trump administration has already invoked the Defense Production Act to get several firms to make mechanical ventilators — although, as we discussed in a recent episode, ventilators haven’t been in as short a supply as predicted; nor do they help Covid-19 patients as much as was anticipated. But, again, in the fog of war decisions are made fast, with much uncertainty and no guarantees. The next logical step, according to Zack Cooper, and just about everyone else we’ve been speaking with, is to boost production of testing very substantially and very fast.
So let’s say that happens. Let’s say Congress gets the message that testing is vital enough to spend $250 billion on, and that there are suddenly millions upon millions of diagnostic and antibody tests available. What happens next? Where, when, and how does all this testing take place? With many hospital systems already under strain from Covid-19, policymakers are talking about building separate infrastructure to deliver testing. But what if that infrastructure already existed?
Steve CHEN: Ninety percent of Americans live within five miles of a pharmacy. And in urban areas, it’s less than 1.8 miles of a pharmacy.
That’s Steve Chen. He’s a practicing pharmacist and also:
CHEN: I’m the associate dean for clinical affairs at the University of Southern California’s School of Pharmacy.
There are roughly 67,000 pharmacies in the U.S., compared to 5,500 hospitals. And how does the training of a pharmacist compare to that of a physician?
CHEN: Pharmacists study to get a four-year doctorate degree after completing an undergraduate degree. So years of training are really no different than physicians and other healthcare professionals that get a formal degree. And then furthermore, when pharmacy students are out in experiential training, they’re training side-by-side with physicians, nurses, other members of the healthcare team. Pharmacists are always there, behind the scenes or sometimes upfront, managing complex, dangerous medications, dosing medications, making recommendations or treatment changes with antibiotics for infectious diseases.
So you might think that pharmacists would be considered “healthcare providers.” Due to a quirk of history, however, they are not.
CHEN: It really starts back with the Social Security Act. In the Social Security Act, healthcare providers are defined and there’s a long list of who is a healthcare provider — everyone, of course, from physicians, all the way down to nurses and chiropractors, nutritionists, psychologists. Pharmacists are not on that list.
The Social Security Act was written in 1935.
CHEN: And back then, pharmacies were thriving businesses. And they did very well with compounding medications. And it was felt to be a critical role. There wasn’t any push at that time to be recognized as a healthcare provider.
But today, that’s more of a problem for pharmacists.
CHEN: You fast forward to today, now, reimbursement from Medicare, reimbursement from Medicaid, from health plans, it’s all tied to who is a provider, officially a provider, in the Social Security Act. So states use that to say, “Hey, we can’t pay pharmacists because they’re not officially healthcare providers.”
Chen and other pharmacist-researchers have done work showing that when pharmacists are actively involved in monitoring and adjusting medications, patient outcomes are considerably improved. But there’s no mechanism that allows them to be compensated for such work. I asked Chen what’s keeping that from happening.
CHEN: So physicians don’t necessarily want to see pharmacists carving into that limited source of funding for healthcare and being paid fee-for-service.
And this has left pharmacists, as Steve Chen describes it, overtrained and underutilized, especially during a crisis like Covid-19. Again, there are more than 10 times as many pharmacies in the U.S. as there are hospitals, with 90 percent of Americans living within five miles of a pharmacy. So: would it maybe be a good idea to authorize pharmacists to administer Covid-19 tests? That’s exactly what the U.S. Department of Health and Human Services decided to do a couple weeks ago.
CHEN: I was pleasantly surprised that it got done because we’re often the forgotten stepchild.
DUBNER: How many Covid tests have been administered in California, where you are, by pharmacists now to date?
CHEN: Zero. Absolutely none.
DUBNER: Because?
CHEN: Any time any authorization occurs at any government level, there’s somewhat of a regulatory process that has to be established. There’s the authorization and there’s a translation of how it actually works and what can be done within each state. And in California that clarity was sought from the Department of Public Health. And the answer we got back is no, pharmacists are not allowed to do Covid testing in California.
That’s even though pharmacists in California can test for diabetes and high cholesterol. These regulations differ widely from state to state. Some states, for instance, allow a pharmacist to adjust medication doses, or even write prescriptions themselves. Other states don’t even allow a pharmacist to take a patient’s temperature. In New York State, governor Andrew Cuomo acted upon the H.H.S. guidance and just authorized the state’s roughly 5,000 pharmacies to conduct Covid-19 testing. As supplies permit, of course.
DUBNER: So pretend for a moment that I am Governor Newsom, governor of California, which has this ruling that forbids pharmacists from administering the Covid test, and you’ve got an audience with me. I say, “Steve Chen, you are a notable figure in the field of pharmacy. Give me your best reasons why it should happen and then tell me the biggest downside.”
CHEN: I would say that there needs to be an exception made because the number of tests for 40 million Californians that you need to get done every day is not going to get done in the current available outlets that you’re thinking of, whether hospitals or clinics or other similar locations. Pharmacists are healthcare professionals. They’re trained. They’ve been able to do this type of testing. And this is not going to be a difficult rollout if you empower pharmacists to be involved.
DUBNER: Well, Professor Chen, that sounds perfectly sensible, but my Department of Health would not have forbidden pharmacists from administering Covid tests were there not a really good reason. What are the reasons why my Department of Health is justified in not having you do these tests?
CHEN: Well, I would say that your Department of Health is reading the law as it’s written, and that’s the problem. You’ve said yourself that we need to make adjustments, be flexible, and allow every healthcare professional to practice at top of licensure in order to beat this infection. And that’s not happening. Pharmacists need to be involved in containing the Covid-19 infection in communities by offering screening, advice, self-management, self-care guidance, quarantine directions, and if needed, referral into the healthcare system, keeping patients from overwhelming emergency rooms and hospitals. And if pharmacists are not deployed in this widespread testing that’s required to lift all these mitigation measures we have out there, I don’t think it’s going to get done.
Okay, so let’s say that pharmacies across the country are enlisted to administer millions upon millions of Covid tests in the coming months, like Steve Chen would like to see. Let’s also say that the federal government comes up with $250 billion to create millions upon millions of Covid tests, like Zack Cooper would like to see. Does that solve the testing problem? Does that clear the way for a smooth and safe exit from quarantine? Not necessarily.
LEVITT: One of the pieces of exiting from the quarantine is that everybody agrees we need to do enormous amounts of tests.
That, again, is Steve Levitt.
LEVITT: What I’m struck by is that no one is talking about the fact that even if we had those tests available, the incentive problem of actually getting people to take those tests is a very difficult one. Somehow people are going to have to be compelled to do those tests. And I think in many cases, you’ll be tested every couple of weeks, even though you have no symptoms. The chances that we’re going be able to get people voluntarily to go down to their pharmacy or whatnot— so I think we have a real incentive problem.
What kind of incentive problem?
LEVITT: This is a classic case of what economists call a negative externality. The costs of me going out on the street when I’m asymptomatic are all borne by other people, right? I infect other people; they get sick. But if I don’t have symptoms— and sometimes the last thing I want to do is go get tested all the time, which is a hassle. Maybe I have to go stand by people who are sick to get tested. And then if I test positive, then I’m quarantined and maybe I lose my job if I’m quarantined. Maybe I can’t afford— you know, I have to pay the rent.
Okay, that does sound like a real incentive problem.
LEVITT: But luckily that’s the kind of problem that economists are really good at. So I think there’s an easy answer to the incentive problem that we can solve, no difficulty at all.
DUBNER: Okay, if the answer is so easy, why don’t you tell us?
LEVITT: Well, I think the answer is: you’ve got to make it worth people’s while to take this test. It’s what economists call “internalizing the externality.” So we’re going to need a lot of apparently healthy people, people without symptoms, to take this test. So I think we should pay them, and a sensible way to do that might be in the form of a really big lottery. So you might even call it, like, Pandemillions, or something like that. So you could imagine we could put something like $500 million, $1 billion a week into this lottery. And in order to get a lottery ticket, you’d have to go and get tested for Covid. And the social benefit would so swamp the costs of doing this. A billion dollars a week or something, it’s peanuts compared to even the existing CARES Act and almost vanishingly small compared to the costs overall of this disease.
DUBNER: What’s the difference if you test positive or negative, though? Do you get more chances at the lottery if you test positive because we want to incentivize people then to stay home for an additional two weeks or whatnot?
LEVITT: So I think if you test positive, it maybe gets simpler because you’re talking about a smaller group of people. I would simply just pay people to stay at home. I would pay a big enough number that even if you don’t feel sick, you’d want to stay home. So if something like, I don’t know, $2,000 per week, and you get paid that as long as you’re testing positive. I would pay handsomely for people to stay at home. I really think if the incentive plans that I’m pushing get put into place, our problem will not be getting people to stay home or to take the test. Our problem will be that people are going to cheat like crazy to try to get certain results and get into the lottery and whatnot. I’d much rather have the problem of people too eager to get tested and faking Covid than the problem we have, which is a pandemic in which people are out and about doing things and we don’t know how to stop it.
How would you respond to Steve Levitt’s Pandemillions idea? Let us know, at radio@freakonomics.com. And if you really like the idea, let your governor know, or someone else in a position to make it happen. Also: remember to subscribe to No Stupid Questions, our new spinoff podcast with Angela Duckworth.
* * *
Freakonomics Radio is produced by Stitcher and Dubner Productions. This episode was produced by Zack Lapinski, with help from Matt Hickey. Our staff also includes Alison Craiglow, Greg Rippin, Daphne Chen, Harry Huggins, and Corinne Wallace; our intern is Isabel O’Brien. We had help this week from James Foster. Our theme song is “Mr. Fortune,” by the Hitchhikers; all the other music was composed by Luis Guerra. You can subscribe to Freakonomics Radio on Apple Podcasts, Stitcher, or wherever you get your podcasts.
Here’s where you can learn more about the people and ideas in this episode:
SOURCES
- Gina Raimondo, governor of Rhode Island
- Dr. Julie Gerberding, former director of the C.D.C. and current chief patient officer for Merck.
- Chris Murray, director of the Institute for Health Metrics and Evaluation.
- Steve Levitt, Freakonomics co-author and economist at the University of Chicago
- Zack Cooper, healthcare economist at Yale University.
- Steve Chen, practicing pharmacist and associate dean at the University of Southern California’s School of Pharmacy.
RESOURCES
- “In New York City, 1 in 7 Expectant Mothers Test Positive for Coronavirus,” by Dena Goffman and Desmond Sutton (Columbia University Irving Medical Center, 2020).
- “Want to know how many people have the coronavirus? Test randomly,” by Daniel N. Rockmore and Michael Herron (The Conversation, 2020).
- “U.S. pharmacists can now test for coronavirus – they could do more if government allowed it,” by Steven W. Chen (The Conversation, 2020).
- “Estimating the cost of vaccine development against epidemic infectious diseases: a cost minimization study,” by Dimitrios Gouglas, Tung Thanh Le, Klara Henderson, Aristidis Kaloudis, Trygve Danielsen, Nicholas Caspersen Hammersland, et al. (Lancet Global Health, 2018).
- “History of 1918 Flu Pandemic,” (Centers For Disease Control and Prevention).
The post How Do You Reopen a Country? (Ep. 416) appeared first on Freakonomics.
Via Finance http://www.rssmix.com/
No comments:
Post a Comment